Finding the best sleeping position for sciatica addresses one of the most disruptive aspects of this condition: nighttime pain that prevents restorative sleep, which in turn slows the neural recovery that determines how quickly sciatic symptoms resolve. The options for sleeping positions for sciatica differ depending on whether the sciatic irritation is from a disc herniation, piriformis syndrome, or lumbar stenosis — because each condition has a different optimal spinal position. Beyond the clinical, people are curious about what your sleeping position says about you — a category of personality-linked sleep position research that has some limited evidence behind it and provides a useful framework for understanding habitual position patterns. The freefall sleeping position — stomach-down with the head turned to one side and arms above or alongside the head — is associated with an open, sensation-seeking personality type in some studies, but is also the position most consistently linked to neck pain and lower back discomfort. Understanding sleep positions meaning in both a physiological and psychological context provides a complete picture of how and why position habits form and what they cost in terms of pain and sleep quality.
This guide covers the science behind sciatica-specific positioning, the evidence for sleep position personality correlates, and how to use that information practically.
Sciatica-Specific Sleeping Positions and Their Mechanisms
Disc-Based Sciatica vs. Piriformis-Based Sciatica
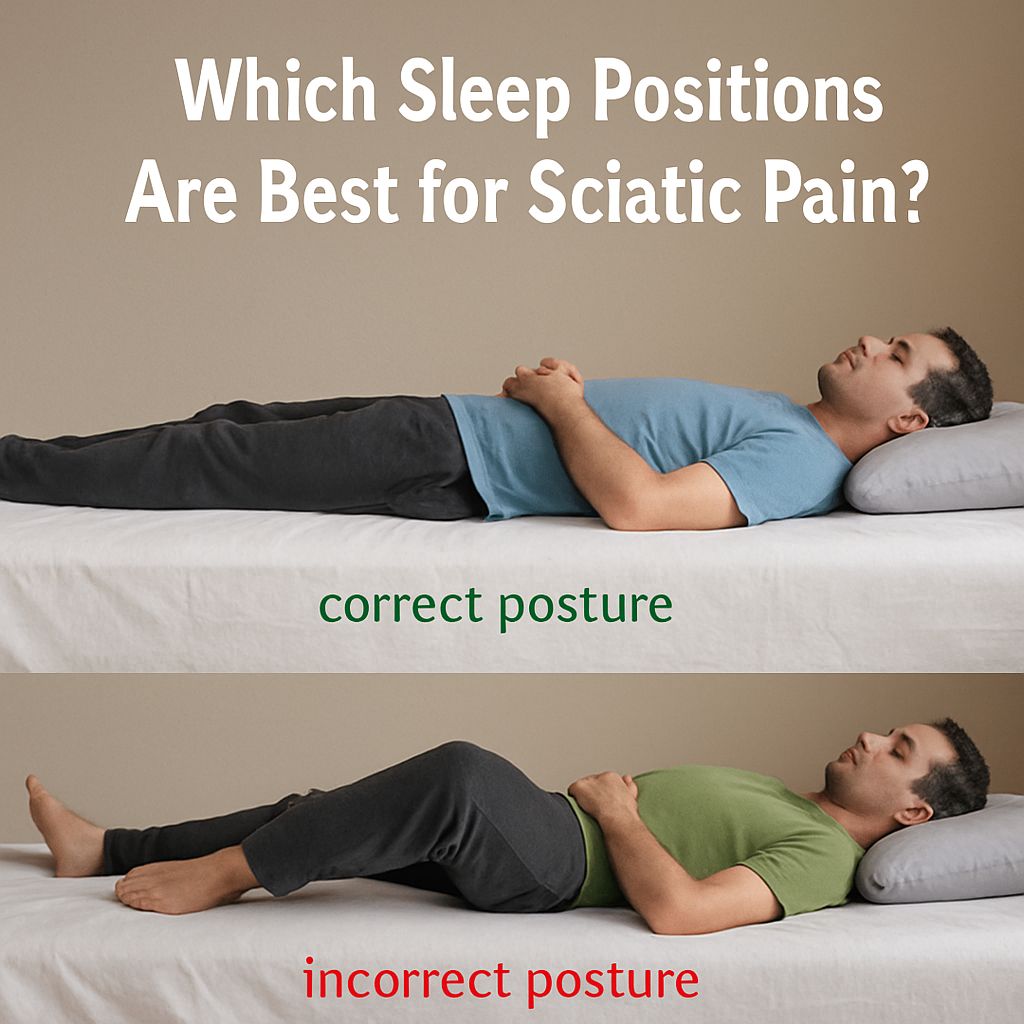
Disc herniation-based sciatica is typically worsened by spinal flexion — bending the spine forward — and improved by mild extension or neutral alignment. This means the fetal curl position favored by side-sleepers often aggravates disc-based sciatica by loading the posterior annulus and increasing the posterior disc bulge that compresses the affected nerve root. The most effective sleeping position for disc-based sciatica is on the side with a pillow between the knees, keeping the spine as neutral as possible — not curled deeply — or back-sleeping with a pillow under the knees, which keeps the lumbar spine in 20 to 30 degrees of flexion rather than full extension.
Piriformis syndrome, where the sciatic nerve is irritated by the piriformis muscle in the posterior hip, responds differently. Internal rotation of the hip — which the fetal curl does not produce — stretches the piriformis across the nerve. External rotation, as occurs when lying on the back with the legs slightly apart or with a small pillow under the affected side’s buttock, reduces piriformis tension and relieves nerve pressure. Distinguishing which mechanism applies requires symptom assessment — disc-based sciatica is worse with sitting and coughing; piriformis-based sciatica is worse with direct hip external rotation.
Sleep Position Personalities and the Freefall Position
The research on sleep position personality links is more epidemiological correlation than mechanistic causation — people who report sleeping in specific positions also report certain personality traits at higher rates, but the link does not imply that position shapes personality or vice versa. The freefall sleeping position, for example, correlates with social boldness and risk-tolerance in self-report surveys, possibly because uninhibited sleepers feel comfortable in an asymmetrical, face-down posture. Whether this reflects genuine trait association or reporting bias is unclear.
From a pain and spinal health perspective, however, the sleep positions meaning is more clinically concrete. The freefall position forces 45 to 90 degrees of cervical rotation for the full sleep duration — the single strongest predictor of recurrent neck pain in all age groups. It also places the lumbar spine in sustained extension and anterior pelvic tilt, loading the facet joints at L4–L5 and L5–S1 in a way that worsens both mechanical low back pain and foraminal stenosis symptoms.
Side-sleepers in a tightly flexed fetal position place the sciatic nerve and its roots in a sustained stretched state that can aggravate existing sciatic irritation. Opening the fetal curl by straightening the hips to a 20 to 30-degree rather than 90-degree angle reduces this stretch while maintaining lateral positioning. Placing a pillow under the waist gap fills the lateral trunk curve and reduces sacroiliac loading simultaneously.
Back-sleepers represent the position associated with the widest spinal canal diameter at each vertebral level — spinal stenosis symptoms are most relieved in this position, and lumbar compressive loads are most evenly distributed. The trade-off is that back-sleeping is the position most strongly associated with snoring and obstructive sleep apnea events, making it a poor universal recommendation for patients with untreated upper airway issues.
Bottom line: The best sleeping position for sciatica depends on whether the nerve irritation is disc-based or piriformis-based — each requires different lumbar and hip positioning. Regardless of sciatica type, the freefall sleeping position is one of the worst options for spinal health and should be phased out with the same systematic positional retraining approach used for any habitual sleep position change.


