Insomnia before period affects a measurable portion of people who menstruate, with studies estimating that 30–40% experience significant sleep disruption in the luteal phase. The hormonal shift from the mid-cycle progesterone peak to the premenstrual drop creates physiological conditions that are genuinely disruptive to sleep architecture, not simply a matter of mood or stress. Understanding the mechanism makes it easier to target the right interventions.
Period insomnia is distinct from general stress-related sleeplessness because it follows a predictable pattern tied to the cycle. Insomnia during period itself is often less severe than the premenstrual phase, as hormone levels begin to equalize. Tracking insomnia period by period using a sleep log or cycle app provides data that both patients and clinicians can use to confirm the relationship. Insomnia art, or the practice of using creative expression to process sleeplessness, has gained attention as a coping mechanism among people who struggle to wind down during this phase.
Hormonal Drivers and Sleep Architecture Changes
Progesterone has a known sedative effect at the cellular level, acting on GABA receptors in ways similar to benzodiazepines. When progesterone drops sharply in the 2–5 days before menstruation, that sedative effect disappears. Body temperature also rises by 0.3–0.5 degrees Celsius in the luteal phase, which interferes with sleep onset because the body needs to drop core temperature by approximately 1 degree to initiate and maintain sleep.
Insomnia before, or sleep disruption leading up to, menstruation tends to reduce slow-wave sleep the most. Slow-wave sleep is the physically restorative stage, and its reduction explains the next-day fatigue and muscle ache that accompany premenstrual sleeplessness. REM sleep is less affected, though vivid dreaming during this phase is common and can contribute to waking.
Tracking the Pattern
Using a cycle tracking app alongside a sleep quality rating each morning, scored on a 1–5 scale, reveals the pattern within two to three cycles. Most people find their worst nights fall consistently in the 2–5 days before menstruation begins. This data makes it possible to plan interventions proactively rather than reacting each month.
Practical Interventions That Target the Luteal Phase
Magnesium glycinate at 300–400 mg taken 60 minutes before bed has clinical support for improving sleep quality during the luteal phase. It works by supporting GABA activity, partially compensating for the progesterone withdrawal effect. Results are typically noticeable within one to two cycles of consistent use.
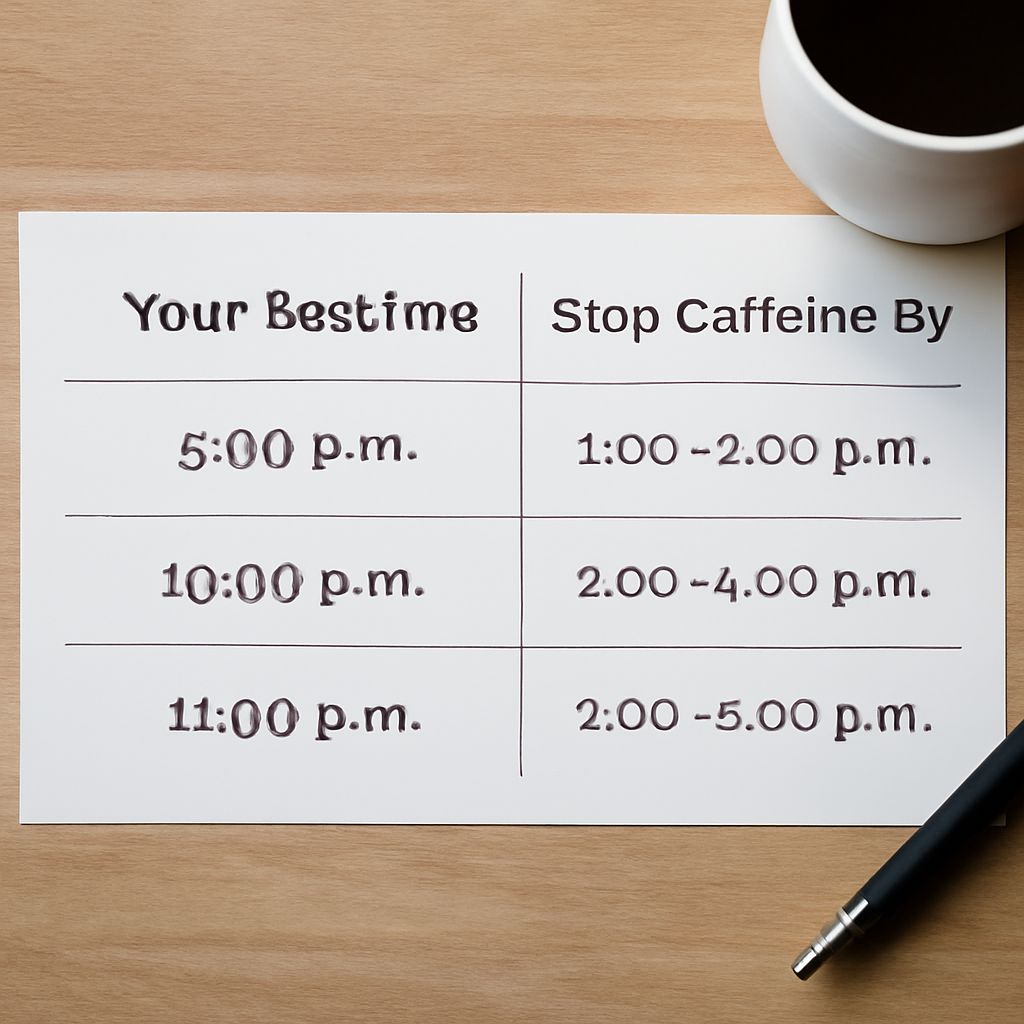
Cooling the sleep environment to 65–68 degrees Fahrenheit counteracts the 0.3–0.5 degree temperature rise and brings the body back within the range that supports sleep onset. A cooling mattress pad or breathable percale bedding achieves this without air conditioning in mild climates. Cutting caffeine by 2 p.m. rather than the usual 4–6 p.m. cutoff during the premenstrual window further reduces sleep latency by 12–18 minutes on average.
Period insomnia also responds to consistent sleep and wake times maintained even on the worst nights, because keeping the circadian anchor intact prevents the spiral where one bad night makes the next one worse. Light exposure of 10,000 lux for 20–30 minutes in the morning helps reset the circadian rhythm and partially compensates for the temperature-driven sleep disruption.