TMJ and Sleep Apnea: Understanding the Link with GERD and Acid Reflux
TMJ and sleep apnea are connected through a relationship that most people — and many clinicians — do not initially consider. The temporomandibular joint governs jaw position during sleep, and when dysfunction causes the jaw to retract, the tongue and soft palate follow, narrowing the airway and increasing the risk of obstructive events. This mechanical pathway means that managing jaw position can sometimes reduce apnea severity even before CPAP therapy is initiated.
GERD and sleep apnea represent a second, equally important connection in sleep medicine. The two conditions affect tens of millions of people simultaneously, with research showing that those with obstructive sleep apnea are three times more likely to have symptomatic acid reflux. Understanding the acid reflux and sleep apnea cycle, how acid reflux sleep apnea patterns develop overnight, and what approaches address sleep apnea and GERD simultaneously improves outcomes for both conditions.
How TMJ Disorders Contribute to Sleep Apnea
The temporomandibular joint sits just in front of the ear and controls the opening, closing, and lateral movement of the jaw. In people with TMJ dysfunction, muscle tension and joint inflammation often cause the mandible to retract during relaxed states — including sleep. This posterior displacement of the jaw pulls the tongue base backward into the pharyngeal airway. Airway cross-sectional area can reduce by 20–30% with even modest mandibular retropositioning.
The connection between TMJ and sleep apnea is bidirectional. Sleep apnea itself causes bruxism — teeth grinding — in approximately 25–50% of affected individuals, due to the arousal response triggered by hypoxic events. The repetitive muscle contractions of bruxism load the TMJ over thousands of cycles per night, accelerating joint wear and muscle fatigue. This feedback loop means untreated sleep apnea worsens TMJ symptoms and vice versa.
Mandibular advancement devices (MADs) — custom oral appliances worn during sleep — address both conditions simultaneously. By advancing the lower jaw 5–10 mm forward, MADs increase pharyngeal airway volume and reduce apnea-hypopnea index (AHI) by an average of 50% in mild-to-moderate OSA. The same forward jaw position reduces TMJ loading by redistributing muscle force more evenly. Dental sleep medicine specialists can titrate MAD advancement at 0.5 mm intervals over four to six weeks until both AHI control and joint comfort are optimized.
The GERD and Sleep Apnea Connection: Mechanisms and Management
The relationship between GERD and sleep apnea operates through several pathways. During obstructive apnea events, the diaphragm contracts forcefully against a closed glottis — a pattern called the Mueller maneuver. This generates strongly negative intrathoracic pressure, which mechanically pulls stomach contents upward through the lower esophageal sphincter. The result is nocturnal reflux triggered not by diet but by the apneic event itself.
The reverse pathway also exists: acid reflux and sleep apnea interact when refluxate reaching the larynx triggers a protective laryngospasm and microarousal. This arousal fragments sleep architecture — reducing slow-wave and REM sleep — and increases the likelihood of subsequent apnea events by destabilizing respiratory control. Patients may experience dozens of these events per night without full awakening, explaining why many report daytime fatigue without remembering waking up.
Acid Reflux Sleep Apnea Treatment Strategies
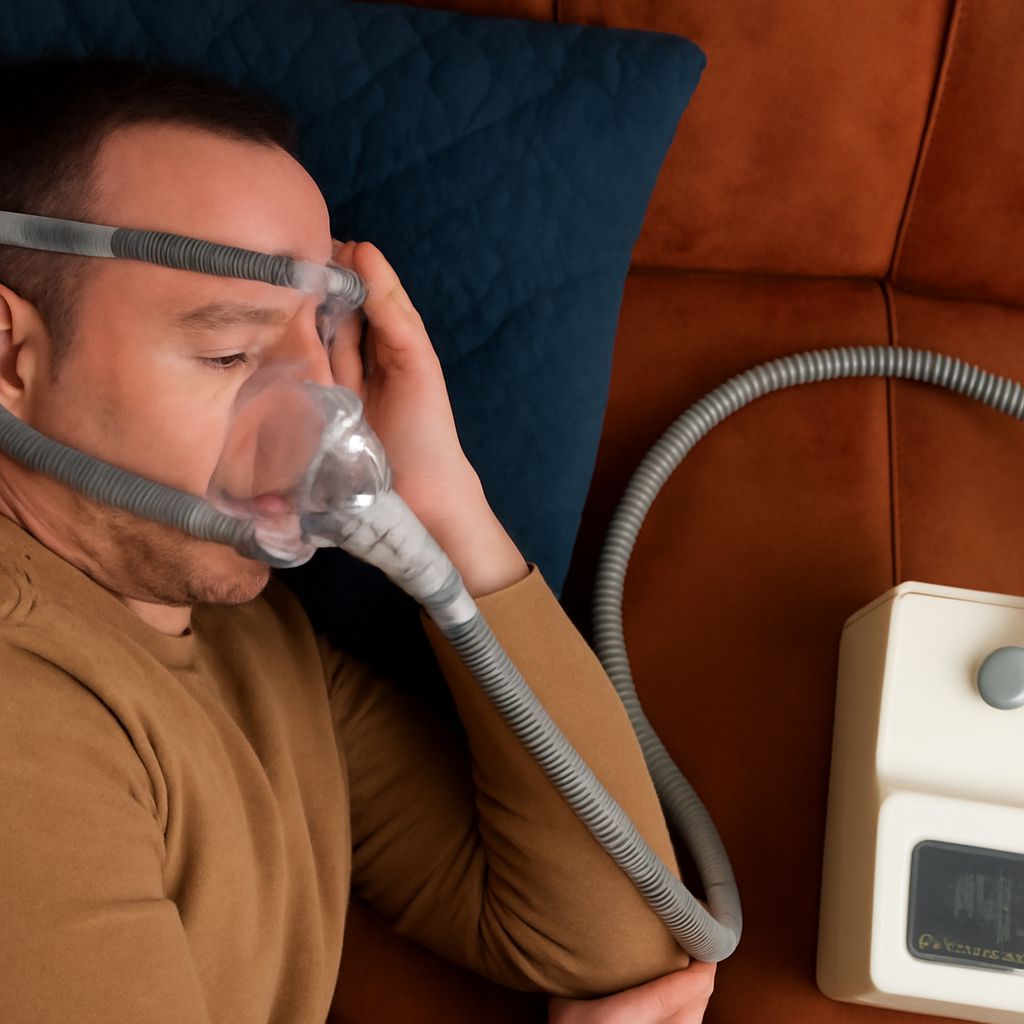
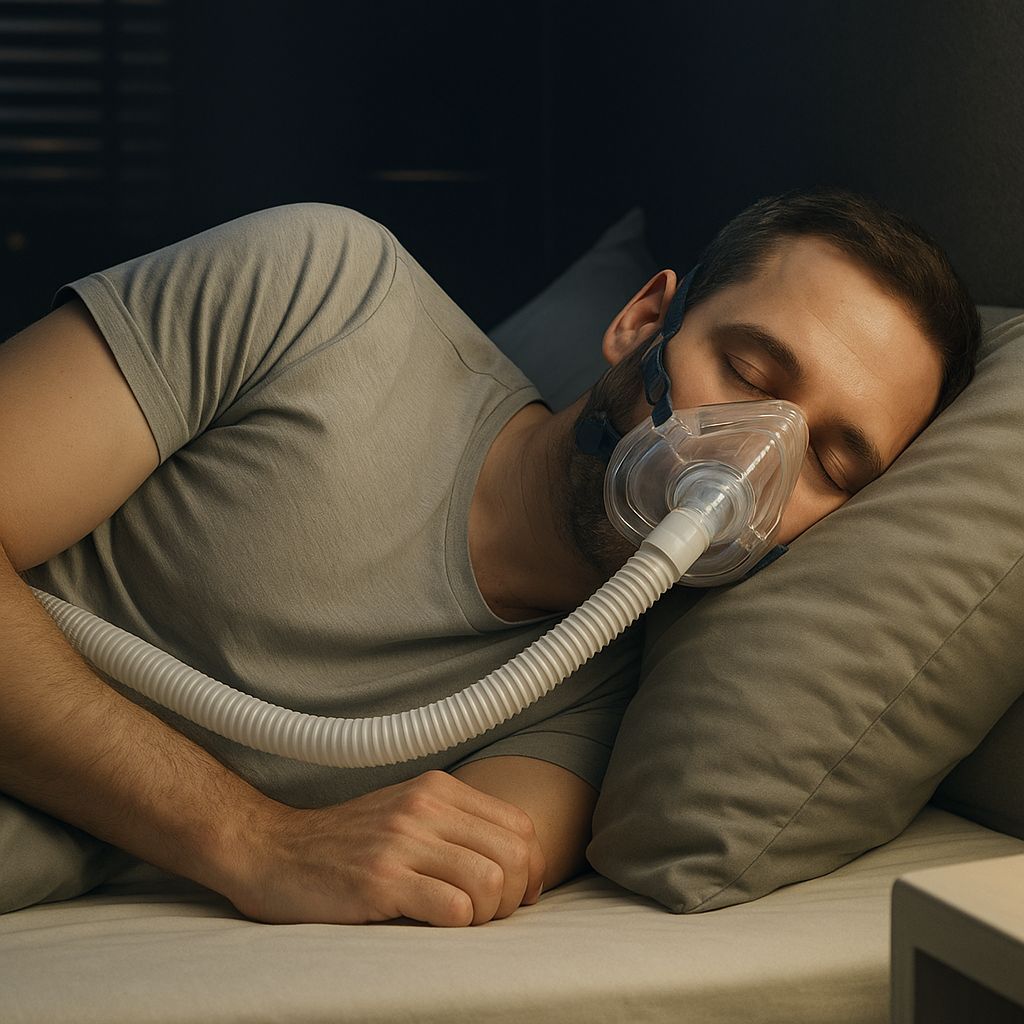
Effective management of the acid reflux sleep apnea cycle requires treating both conditions, ideally simultaneously. CPAP therapy reduces reflux events by 40–60% in patients with concurrent sleep apnea and GERD — the positive pressure stabilizes the lower esophageal sphincter by reducing the pressure gradient across it. This means that initiating CPAP often improves GERD symptoms even before any dietary changes are made.
Positional therapy reinforces CPAP benefits. Elevating the head of the bed by 6–8 inches — using a wedge pillow or bed risers rather than extra pillows, which flex the neck — reduces gravitational acid migration. Left-side sleeping further reduces reflux events by positioning the gastroesophageal junction above the gastric pool, reducing acid contact time with the esophageal mucosa by up to 70% compared to right-side lying.
Proton pump inhibitors (PPIs) taken 30–60 minutes before the largest meal of the day reduce acid production and are the first-line pharmacological treatment for sleep apnea and GERD. However, PPIs do not address the mechanical pressure pathway triggered by apneic events — only treating the apnea itself achieves that. For this reason, combination therapy consistently outperforms either treatment alone in clinical trials measuring both nocturnal AHI and GERD symptom scores.
Dietary timing matters significantly. Eating the last meal at least three hours before lying down gives gastric contents time to partially empty. Avoiding high-fat meals in the evening reduces gastric emptying delay, which otherwise increases the overnight reflux window. Alcohol reduces lower esophageal sphincter tone and increases apnea frequency through central respiratory depression — eliminating alcohol within four hours of sleep addresses both conditions simultaneously.
Next steps: Anyone with both acid reflux and sleep-related symptoms should request a polysomnography referral rather than treating each condition separately. Confirming and treating sleep apnea often resolves GERD symptoms that have resisted dietary and pharmacological management for years. A dental sleep medicine consultation is additionally worthwhile when TMJ symptoms accompany the sleep apnea diagnosis.